Introduction:
- The larynx is the organ for production of voice or phonation.
- It is also an air passage, and acts as a sphincter at the inlet of the lower respiratory passages.
- The upper respiratory passages include the nose, the nasopharynx and the oropharynx.
- Larynx or voice box is well developed in humans.
- Its capabilities are greatly enhanced by the large "vocalisation area" in the lower part of motor cortex.
- Our speech is guided and controlled by the cerebral cortex.
- Larynx is a part of the respiratory system allowing two way flow of gases.
- It is kept patent because an adult is breathing about 15 times per minute, unlike the oesophagus which opens at the time of eating or drinking only.
SITUATION AND EXTENT
The larynx lies in the anterior midline of the neck extending from root of tongue to trachea
In adult male, it lies in front of C3 to C6 vertebrae but in children and adult female it lies at a little higher level.
SIZE
The length of the larynx is 44 mm in males and 36 mm in females.
At puberty, the male larynx grows rapidly and becomes larger, seen as prominent angle
of thyroid cartilage( adam’s apple),
which makes voice louder and low pitched.
The pubertal growth the female larynx is negligible, and her voice is high pitched.
Internal diameter up to 3 yrs it is 3 mm and adult it is 12 mm.

CONSTITUTION OF LARYNX
The larynx is made up of a skeletal framework of cartilages
The cartilages are connected by joints, ligaments and membranes
are moved by number of muscles
The cavity of larynx is lined by mucous membrane
Cartilages of larynx
The larynx contains nine cartilages, of which three are unpaired and three, paired.
Unpaired Cartlages
1. Thyroid (Greek shield like)
2. Cricoid (Greek ring like)
3. Epiglottis (Greek leaf like)
Paired Cartilages
1. Arytenoid (Greek cup shaped)
2. Corniculate (Latin horn shaped) 3. Cuneiform (Latin wedge shaped)

Thyroid Cartilage
- This cartilage is V-shaped in cross-section.
- It consists of right and left laminae
- Each lamina is roughly quadrilateral.
- The laminae are placed obliquely relative to
the midline, their posterior borders are far apart, but the anterior borders approach each other at an angle that is about 90 degrees in the male and about 120 degrees in the female. - The lower parts of the anterior borders of the right and left laminae fuse and form a median projection called the laryngeal prominence.
- The upper parts of the anterior borders do not meet.
- They are separated by the thyroid notch.
- The posterior borders are free.
- They are prolonged upwards and downwards
as the superior and inferior cornua or horns.


The superior cornua is connected with the greater cornua of the hyoid bone by the lateral thyrohyoid ligament.
The inferior cornua articulates with the cricoid cartilage to form the cricothyroid joint
The inferior border of the thyroid cartilage is convex in front and concave behind.
In the median plane, it is connected to the cricoid cartilage by the conus elasticus.
The outer surface of each lamina is marked by an oblique line which extends from the superior thyroid tubercle in front of the root of superior cornua to the inferior thyroid tubercle behind the middle of inferior border.

Attachments
- The (i) thyrohyoid, (ii) sternothyroid and (iii) thyropharyngeus part of inferior constrictor of pharynx are attached to the oblique line.
- Lower border and inferior cornua gives insertion to triangular cricothyroid.
- Along the posterior border connecting superior and inferior cornua is the insertion of
(i) palatopharyngeus, (ii) salpingopharyngeus, (iii) stylopharyngeus
- a. Median thyroepiglottic ligament,
- b. Thyroepiglottic muscle on each side,
- c. Vestibular fold on each side,
- d. Vocal fold on each side,
- e. Thyroarytenoid and
- f. Vocalis muscle on each side

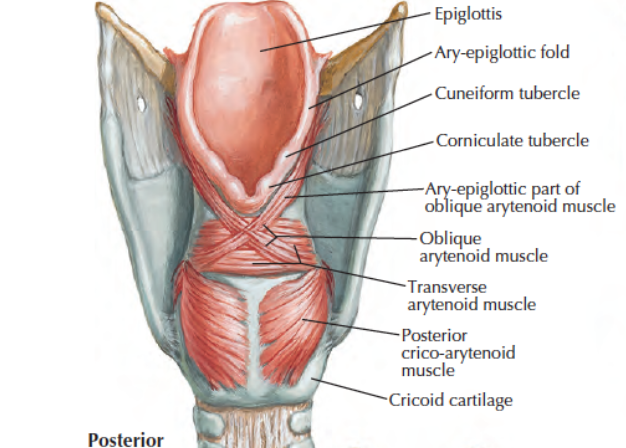
Cricoid Cartilage
This cartilage is shaped like a ring.
It encircles the larynx below the thyroid cartilage and forms foundation stone of larynx.
It is thicker and stronger than the thyroid cartilage.
The ring has a narrow anterior part called the arch,
and a broad posterior part, called the lamina The lamina projects upwards behind the thyroid cartilage,
articulates superiorly with the arytenoid cartilages.
The inferior cornua of the thyroid cartilage articulates with the side of the cricoid cartilage at the junction of the arch and lamina.

Attachments
Anterior part of arch of cricoid gives origin to triangular cricothyroid muscle, a tensor of vocal cord.
Anterolateral aspect of arch gives origin to lateral cricoarytenoid muscle, an adductor of vocal cord.
Lamina of cricoid cartilage on its outer aspects gives origin to a very important "safety muscle", the posterior cricoarytenoid muscle. Cricothyroid and quadrate membranes are also attached.

Epiglottis
This is a leaf-shaped cartilage placed in the anterior wall of the upper part of the larynx.
Its upper end is broad and free, and projects upwards behind the hyoid bone and the tongue
The lower end or thyroepiglottic ligament is pointed and is attached to the upper part of the angle between the two laminae of the thyroid cartilage

Attachments
The right and left margins of the cartilage provide attachment to the aryepiglottic folds
lts anterior surface is connected:
a. To the tongue by a median glossoepiglottic fold
b. To the hyoid bone by the hyoepiglottic ligament
The posterior surface is covered with mucous membrane, and presents a tubercle in the lower part.
Thyroepiglottic muscle is attached between thyroid cartilage and margins of epiglottis.
It keeps the inlet of larynx patent for breathing.
Aryepiglottic muscle closes inlet during swallowing

Arytenoid cartilage
These are two pyramidal shaped cartilages lying on the upper border of lamina of thyroid cartilage
The apex is curved posteromedially and articulates with corniculate cartilage
Its base is concave and articulates with the lateral part of upper border of cricoid lamina
It is prolonged anteriorly to form vocal process
It is prolonged laterally to form muscular process
Its surfaces are 1. anterolateral, 2. medial and 3. posterior

Attachments
Vocal process: Vocal fold and vocalis muscle is attached.
Above vocal process; Vestibular fold attached.
Muscular process:
Posterior aspect gives insertion to posterior cricoarytenoid.
Anterior aspect gives insertion to lateral cricoarytenoid.
Posterior surface -
Transverse arytenoid across the two cartilages. Between base and apex of arytenoid is oblique arytenoid which continue s as aryepiglottic muscle into two sides of epiglottis.
Quadrangular or quadrate membrane is attached between arytenoid, epiglottis and thyroid cartilages

Corniculate Cartilages
These are two small conical nodules which articulate with the apex of the arytenoid cartilages, and
are directed posteromedially.
They lie in the posterior parts of the aryepiglottic folds
Cuneiform Cartilages
These are two small rod-shaped pieces of cartilage placed in the aryepiglottic folds just ventral to the corniculate cartilages


Histology of Laryngeal Cartilages
The thyroid, cricoid cartilages, and the basal parts of the arytenoid cartilages are made up of the hyaline cartilage.
They may ossify after the age of 25 years.
The other cartilages of the larynx, e.g. epiglottis, corniculate, cuneiform and processes of the arytenoid are made of the elastic cartilage and do not ossify
Laryngeal Joints
The cricothyroid joint is a synovial joint
between the inferior cornua of the thyroid cartilage and the side of the cricoid cartilage.
It permits rotatory movements around a transverse axis passing through both cricothyroid joints permitting tension and relaxation of vocal cords. There is some gliding movement also in
The cricoarytenoid joint is also a synovial joint between the base of the arytenoid cartilage and the upper border of the lamina of the cricoid cartilage.
It permits rotatory movements around a vertical axis permitting adduction and abduction of the vocal cords and also gliding movements in all directions

Laryngeal Ligaments and Membranes
Extrinsic
1. The thyrohyoid membrane connects the thyroid cartilage to the hyoid bone.
Its median and lateral parts are thickened to form the median and lateral thyrohyoid ligaments.
The membrane is pierced by the internal laryngeal nerve, and by the superior laryngeal vessels.
2. The hyoepiglottic ligament connects the upper end of the epiglottic cartilage to the hyoid bone.
3. The cricotracheal ligament connects the cricoid cartilage to the upper end of the trachea

Intrinsic
- The intrinsic ligaments are part of a broad sheet of fibroelastic tissue, known as the fibroelastic membrane of the larynx.
- This membrane is placed just outside the mucous membrane.
- It is interrupted on each side by the sinus of the larynx.
- The part of the membrane above the sinus is known as the quadrate membrane, and
- the part below the sinus is called the conus elasticus
- The quadrate membrane extends from the arytenoid cartilage to the epiglottis.
- It has a lower free border which forms the vestibular fold
and an upper border which forms the aryepiglottic fold. - The conus elasticus or cricovocal membrane extends upwards and medially from the arch of the cricoid cartilage.
- The anterior part is thick and is known as the cricothyroid ligament.
- The upper free border of the conus elasticus forms the vocal fold

Cavity of Larynx
1. The cavity of the larynx extends from the inlet of the larynx to the lower border of the cricoid cartilage.
The inlet of the larynx is placed obliquely.
It looks backwards and upwards, and opens into the laryngopharynx.
The inlet is bounded anteriorly, by the epiglottis; posteriorly, by the interarytenoid fold
of mucous membrane; and on each side, by the aryepiglottic fold.
Internal diameter: Up to 3 years - 3 mm;
every year it increases by 1 mm up to 12 years.

Within the cavity of larynx, there are two folds of mucous membrane on each side.
The upper fold is the vestibular fold,
and the lower fold is the vocal fold.
The space between the right and left vestibular folds
is the rima vestibuli; and
the space between the vocal folds is the rima glottidis
The vocal fold is attached anteriorly to the middle of the angle of the thyroid cartilage on its posterior aspect; and posteriorly to the vocal process of the arytenoid cartilage.
The rima glottidis is limited posteriorly by an interarytenoid fold of mucous membrane.
The rima, therefore, has an anterior intermembranous part (three-fifth) and a posterior intercartilaginous part.
The rima is the narrowest part of the larynx.
It is longer (23 mm) in males than in females (17 mm).


The vestibular and vocal folds divide the cavity of
the larynx into three parts.
a. The part above the vestibular fold is called the vestibule of the larynx or supraglottis.
b. The part between the vestibular and vocal folds is called the sinus or ventricle of the larynx
c. The part below the vocal folds is called the infraglottis
The sinus of Morgagni or ventricle of the larynx is a narrow fusiform cleft between the vestibular and vocal folds.
The anterior part of the sinus is prolonged upwards as a diverticulum between the vestibular fold
and the lamina of the thyroid cartilage.
This extension is known as the saccule of the larynx .
The saccule contains mucous glands which help to lubricate the vocal folds.
It is often called oil can of larynx.

Mucous Membrane of larynx
1. The anterior surface and upper half of the posterior surface of the epiglottis, the upper parts of the aryepiglottic folds, and the vocal folds are lined by the stratified squamous epithelium.
The rest of the laryngeal mucous membrane is covered with the ciliated columnar epithelium
2. The mucous membrane is loosely attached to the cartilages of the larynx except over the vocal ligaments and over the posterior surface of the epiglottis where it is thin and firmly adherent.
3. The mucous glands are absent over the vocal cords,
but are plentiful over the anterior surface of the epiglottis, around the cuneiform cartilages and in the vestibular folds.
The glands are scattered over the rest of the larynx.
Clinical Anatomy
- Since the larynx or glottis is the narrowest part of the respiratory passages, foreign bodies are usually lodged here.
- Infection of the larynx is called laryngitis. It is characterized by hoarseness of voice.
- Laryngeal oedema may occur due to a variety of causes. This can cause obstruction to breathing.
- Misuse of the vocal cords may produce nodules on the vocal cords mostly at the junction of anterior one-third and posterior two-thirds.
These are called Singer's nodules or Teacher's nodules - Fibreoptic flexible laryngoscopy : Under local anaesthesia flexible laryngoscope is passed and larynx well visualised.
- Microlaryngoscopy: This procedure is performed under operating microscope. Vocal cord tumors and diseases are excised by this method.
- External examination of larynx: Head is flexed in sitting position. Examiner stands behind and palpates larynx and neck with finger tips for tumour, swelling, lymphadenitis, etc.
- Speech analysis is also necessary in laryngeal diseases.
- Foreign body in larynx: At times fishbones may get impacted in the vallecula or piriform fossa. Often these bones just scratch the mucosa on their way dowry and the person gets a feeling of foreign body sensation, due to a dull visceral pain caused by the scratch.
- Piriform fossa lies between quadrate membrane and medial side of thyroid cartilage. It is traversed by internal laryngeal nerve.
Piriform fossa is used to smuggle out precious stones, diamonds, etc. It is called smuggler's fossa - The mucous membrane of the larynx is supplied by X nerve through superior laryngeal or recurrent laryngeal nerves. So laryngeal tumours may also cause referred pain in the ear partly
- Large foreign bodies may block laryngeal inlet leading to suffocation.
- Small foreign bodies may lodge in laryngeal ventricle, cause reflex closure of the glottis and suffocation.
- Inflammation of upper larynx may cause oedema of supraglottis part. It does not extend below vocal cords because mucosa is adherent to vocal ligament.
Intrinsic Muscles of the larynx
Cricothyroid
The only muscle outside the larynx
Origin: Lower border and lateral surface of cricoid
Fibres pass backwards and upwards
Insertion: lnferior cornua and lower border of thyroid cartilage
lt is called 'tuning fork of larynx’
Nerve Supply - External laryngeal nerve
Action - Tensor of vocal cord and modulation of voice

Posterior cricoarytenoid
triangular
Origin - Posterior surface of the lamina of cricoid
Upwards and laterally
Insertion - Posterior aspect of muscular process of arytenoid
Nerve Supply - Recurrent Laryngeal Nerve
Action - The only Abductor of vocal cord

Lateral cricoarytenoid
Origin - Lateral part of upper border of arch of cricoid
Upwards and backwards
Insertion - Anterior aspect of muscular process of arytenoid
Nerve Supply - Recurrent Laryngeal Nerve
Action - Adductor of vocal cords

Transverse arytenoid
Unpaired muscle
Origin - Posterior surface of one arytenoid
Transverse
Insertion - Posterior surface of another arytenoid
Nerve Supply - Recurrent Laryngeal Nerve
Action - Adductor of vocal cords

Oblique arytenoid and aryepiglottic
Origin - Muscular process of one arytenoid Oblique
Insertion - Apex of the other arytenoid. Some fibres are continued as aryepigloftic muscle to the edge of the epiglottis
Nerve Supply - Recurrent Laryngeal Nerve
Action - Oblique arytenoid - Adductor of vocal cords
aryepiglottic - Closing of inlet of larynx

Thyroarytenoid and thyroepiglottic
Origin - Thyroid angle and adjacent cricothyroid ligament
Backwards and upwards
Insertion - Anterolateral surface of arytenoid cartilage.
Some of the upper fibres of thyroarytenoid curve upwards into the aryepiglottic fold to reach the edge of epiglottis, known as thyroepiglottic
Nerve Supply - Recurrent Laryngeal Nerve
Action - Thyroarytenoid - Relaxor of vocal cords
thyroepiglottic - opening inlet of larynx

Vocalis
Origin - Vocal process of arytenoid cartilage Pass forwards
Insertion - Vocal ligament and thyroid angle
Nerve Supply - Recurrent Laryngeal Nerve
Action - Relaxor of vocal cords

Movements of vocal cords/ folds
Movements of the vocal folds affect the shape and size of the rima glottidis.
1. During quiet breathing or condition of rest, the intermembranous part of the rima is triangular, and the intercartilaginous part is quadrangular
2. During phonation or speech, the glottis is reduced to a chink by the adduction of the vocal folds
3. During forced inspiration, both parts of the rima are triangular, so that the entire rima is lozenge shaped;
the vocal folds are fully abducted
(i.e. diamond shaped glottis).
4. During whispering, the intermembranous part of the rima glottidis is closed, but the intercartilaginous part is widely open(i.e. funnel shaped glottis)

Nerve Supply
Motor Supply
Recurrent laryngeal nerve supplies posterior cricoarytenoid, lateral cricoarytenoid, transverse and oblique arytenoid, aryepiglottic, thyroarytenoid, thyroepiglottic muscles.
It supplies all intrinsic muscles except cricothyroid.
External laryngeal nerve only supplies cricothyroid muscle. Sensory Supply
The internal laryngeal nerve supplies the mucous membrane up to the level of the vocal folds.
The recurrent laryngeal nerve supplies it below the level of the vocal folds. Lymphatic Drainage
Lymphatics from the part above the vocal folds drain along the superior thyroid vessels to the anterosuperior group of deep cervical nodes by piercing thyrohyoid membrane.
Those from the part below the vocal folds drain to the posteroinferior group of deep cervical nodes. A few of them drain into the prelaryngeal nodes by piercing cricothyroid
Clinical Anatomy
- The larynx can be examined either directly through a laryngoscope (direct laryngoscopy); or indirectly through a laryngeal mirror (indirect laryngoscopy).
- By laryngoscopy, one can inspect the base of the tongue, the valleculae, the epiglottis, the aryepiglottic folds, the piriform fossae, the vestibular folds, and the vocal folds.
- Tumours of the vocal cords can be diagnosed early, because there are changes in the voice.
- Tumours in subglottic area present late so are diagnosed late and have poor prognosis.
- Laryngotomy; The needle is inserted in the midline of cricothyroid membrane, below the thyroid prominence. This is done as an emergency procedure.
- Tracheostomy is a permanent procedure. Part of 2nd-4th rings of trachea are removed after incising the isthmus of the thyroid gland.
- If the patient is unconscious, one must remember A-Airway, B-Breathing, C-Circulation in that order. For the patency of airway, pull the tongue out and also endotracheal tube needs to be passed.
- The tube should be passed between the right and left vocal cords down to the trachea.
INFANT'S LARYNX
Cavity of infant's larynx is short and funnel-shaped. Size is one-third of an adult. Lumen is very narrow.
Position is higher than in adult.
Epiglottis lies at C2 and during elevation, it reaches C1, so that infant can use nasal airway for breathing while suckling.
Laryngeal cartilages are softer, more pliable than in adult. Thyroid cartilage is shorter and broader.
Vocal cords are only 4-4.5 mm long, shorter than in childhood and in adult. Supraglottic and subglottic mucosa are lax, swelling results in respiratory obstruction. One must be careful while giving anaesthesia to an infant (birth to one year).
Clinical Anatomy
When any foreign object enters the larynx severe protective coughing is excited to expel the object. However, damage to the internal laryngeal nerve produces anaesthesia of the mucous membrane in the supraglottic part of the larynx breaking the reflex arc so that foreign bodies can readily enter it.
Damage to the external laryngeal nerve causes some weakness of phonation due to loss of the tightening effect of the cricothyroid on the vocal cord.
When both recurrent laryngeal nerves are interrupted, the vocal cords lie in the cadaveric position in between abduction and adduction and phonation is completely lost.
Deep breathing also becomes difficult through the partially opened glottis.
When only one recurrent laryngeal nerve is paralysed, the opposite vocal cord compensates for it and phonation is possible but there is hoarseness of voice.
There is failure of forceful explosive part of voluntary and reflex coughing
Tumours in the piriform fossa cause dysphagia.
These also cause referred pain in the ear. Pain of pharyngeal tumours may be referred to the ear, as X nerve carries sensation both from the pharynx and the external auditory meatus and the tympanic membrane.
Recurrent laryngeal nerve: Mediastinal tumours may press on the left recurrent laryngeal nerve, as it is given off in the thorax. The pressure on the nerve may present as alteration in the voice.
Right recurrent laryngeal nerve is given off in the neck, so it is not affected by mediastinal tumours.
No comments:
Post a Comment